Three Major Red Flags in Minnesota’s Assisted Suicide Bill: Prohibitions, Requirements, and Loopholes
Assisted suicide advocates in Minnesota, such as the group Compassion & Choices, use terms such as “medical aid in dying” to describe doctors enabling patients to end their own lives. However, to understand better what assisted suicide advocates wish to see happen, we must take a closer look at the legislation they support.
In Minnesota, Compassion & Choices has backed a bill (SF 1572 / HF 1885) that would legalize assisted suicide in Minnesota. Yet, this bill contains prohibitions, requirements, and loopholes that serve to advance the agenda of Compassion & Choices at the cost of providing patients with real medical care and putting physicians at risk of abuse and coercion.
1. Minnesota’s Assisted Suicide Bill Prohibits Factual Language
Assisted Suicide as defined by Derek Humphry, Founder of Final Exit Network & forefather of Compassion & Choices: “You get lethal drugs from somebody else, usually a physician, and swallow them to cause your death.”
Derek Humphry, founder of the Hemlock Society (now Compassion & Choices), defines assisted suicide in his book “Final Exit” – a how-to guide on assisted suicide. He defines assisted suicide by saying, “You get lethal drugs from somebody else, usually a physician, and swallow them to cause your death.”
The language in Minnesota’s bill allows doctors to write prescriptions for lethal dosages of drugs so “qualified patients” can intentionally overdose and end their own lives. This is how Humphry himself – the forefather of Compassion & Choices -defined assisted suicide.
Humphry’s definition may seem blunt and callous. It’s also not exactly the best image for Compassion & Choices to build support.

A closer examination of Minnesota’s assisted suicide bill reveals disturbing prohibitions, requirements, and loopholes.
So, in an attempt to change their image, the group wants to prohibit the use of the term “assisted suicide” in public reports. Instead, Minnesota’s bill requires the use of the term “medical aid in dying.” (See Subd. 16. C)
One can see in the language used in Minnesota’s bill that Compassion & Choices supports changing what it means to provide “medical” care. But, the reality is, simply calling something by a different name does not change what it is. Assisted suicide intentionally helps to cause someone’s death. Medical care should never do this.
The fact of the matter is “medical aid in dying” and “assisted suicide” are no different. The former uses couched language that creates a façade of providing medical care. The reality is that intentionally giving patients lethal overdoses of drugs, so patients can swallow them to end their lives, is a manipulation of what it means to provide medical care. Causing death is not medical care.
Changing a term from “assisted suicide” to “medical aid in dying” may seem benign. But, the prohibition of the term “assisted suicide” and the requirement to call it a form of medical care will not serve the common good of patients who deserve true medical care.

When death is cheap, but care is not, what kind of choice is that?
When death becomes an acceptable form of “medical care,” too often insurers treat real care as a choice that is too expensive. While many of these cases will go untold, testimonies from Dr. Brian Callister and Barbara Wagner show us that when assisted suicide becomes a legal option, coverage for treatments are rationed or even refused.
By prohibiting the term “assisted suicide” and requiring it to be called a form of medical treatment, the only party that is served is Compassion & Choices. However, this attempt to alter language does not alter reality. “Medical aid in dying” will always be assisted suicide. Period.
2. Minnesota’s Assisted Suicide Bill Requires Falsified Death Certificates
Physicians are often the ones to verify cause of death on a patient’s death certificate. However, Minnesota’s bill tells physicians to falsify that section when the patient dies by assisted suicide. The bill states in subdivision 17, “The qualified patient’s underlying terminal illness shall be listed as the cause of death.”
At first glance, there seems to be some logic to this. By listing the underlying cause as being cancer or ALS, it would seem this could help to show health trends which impact public health funding, among other items. For example, a public health officials looking at a death certificate should be able to see if a given disease has increased or decreased in a given population.
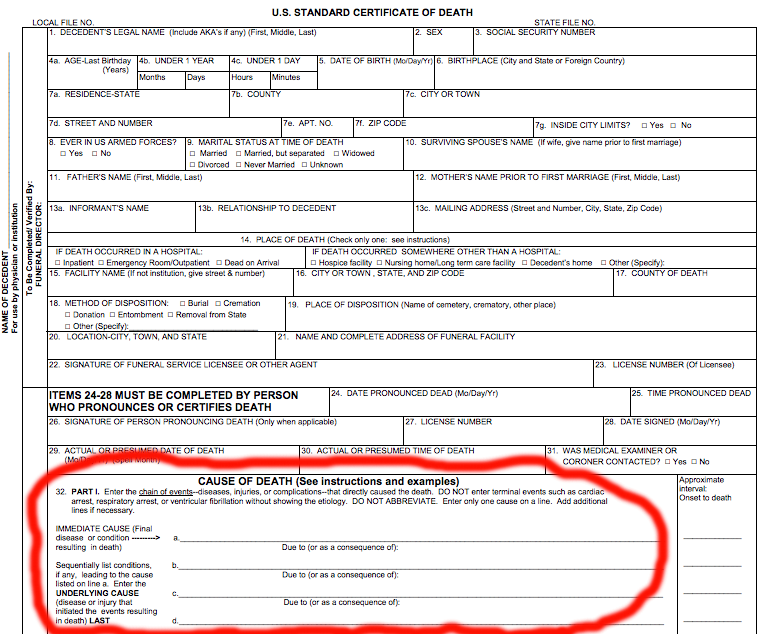
The death certificate should list both immediate cause of death and any underlying causes of death. By listing assisted suicide as the immediate cause of death, it does not negate listing underlying causes.
However, upon further investigation, we find that death certificates already show what underlying causes have led up to a patient’s death. For example, if a patient ultimately dies of respiratory failure, the certificate would have listed underlying causes such as pneumonia preceded by lung cancer that was brought on by years of smoking.
Now, if a cancer patient decides at the onset of pneumonia to ingest assisted suicide drugs, the logical outcome would actually be to list the cause of death as assisted suicide by an overdose of barbiturates (the assisted suicide drugs). Yet, Minnesota’s bill goes against this logic. It instead requires listing the underlying cause (cancer or pneumonia) as the cause of death.
To report the factual cause of death – assisted suicide by an overdose of barbiturates – does nothing to prevent listing the underlying causes that led to the patient taking his or her life. However, the requirement to not list the underlying cause instead of assisted suicide, leaves out vital information.
The Centers for Disease Control and Prevention explains the importance of accuracy in reporting a patient’s cause-of-death:
![]() “Cause-of-death information is used to detect trends … that determine public health programs and health care funding allocations. Aside from the public health significance, it is part of a permanent legal record. Physicians must use their best medical judgment to determine the cause-of-death.”
“Cause-of-death information is used to detect trends … that determine public health programs and health care funding allocations. Aside from the public health significance, it is part of a permanent legal record. Physicians must use their best medical judgment to determine the cause-of-death.”
Without this information, there is no way to tell whether there is a surge or a pocket of patients prematurely ending their lives through assisted suicide. Without that knowledge, it cannot be known if providers are targeting a particular population for the cheaper assisted suicide option instead of providing real care options which may be costlier. This could be a strong factor in patients deciding where they seek medical treatment.
Without this information, there is no way to know if patients with a particular disease are more likely to end their lives by assisted suicide. If that could be known, it could answer questions of whether that population is more susceptible to depression or perhaps facing undue pain towards the end of life. With that knowledge, proper funding could be given to provide these types of patients with care that meets their end-of-life needs.
For the sake of public health, the proper allocation of funding, and the overall common good of patients, factual reporting is vital. To require the falsification of death certificates only covers up the facts.
3. Loopholes in Minnesota’s Assisted Suicide Bill Fail to Protect Physicians’ Conscience Rights

Why should the law force a doctor to choose between losing her job and referring a patient for assisted suicide?
If someone told their neighbor how to get lethal drugs, knowing that neighbor wanted to end his life with those drugs, it would be normal to view the person as knowingly participating their neighbor’s death. This illustrates that when doctors feel that referring a patient to get assisted suicide drugs is “participating” in the patient’s death, it is not abnormal.
No one, in good conscience, would force you to tell your neighbor how to get lethal drugs. It seems only logical that you should have the right to not participate in something that your conscience tells you is wrong. Yet, if you are a doctor and that neighbor is now your patient, Minnesota’s assisted suicide bill does not provide common sense conscience rights protections.
It clearly states (in Subd. 14) that referring a patient to a participating physician (someone who will give them assisted suicide drugs) cannot be considered “participation” in assisted suicide. By excluding referrals from the definition of “participation,” it leaves the door wide open for abuse. This law could force physicians, other medical professionals, and even entire healthcare facilities into providing referrals or face losing their jobs, fighting lawsuits, or worse.
This bill may not hold the first physician, who provides the referral, legally responsible for the patient’s death, but it fails to protect physicians who cannot in good conscience help patients to kill themselves. Without protections for the conscience rights of medical professionals, employers can fire them, and patients can file lawsuits against individuals or even an entire healthcare facility.
Compromising an individual’s livelihood or the future of an entire healthcare facility are clears factors could easily force them to provide a referral even against their conscience. You could lose your local clinic or doctor because they stand up for providing real care and against participation in assisted suicide.
So, despite this bill stating that “participation” in assisted suicide would be completely voluntary, it is clear that the bill’s definition of “participation” would fail to protect the conscience rights of medical professionals and healthcare facilities, that view referrals as participation.
One’s ability to provide real care to patients should not be dependent on whether they are willing to compromise what they know in their conscience to be right. The law must protect medical providers and healthcare facilities which does not wish to participate in assisted suicide – including referrals – whether for ethical or other reasons. Minnesotans must stand up against coercive forces that would cause medical providers to chose between their consciences and their livelihoods.
Minnesotans Deserve Laws that Protect and Uphold the Truth
Keep assisted suicide out of Minnesota.
Minnesotans deserve real care throughout life’s journey, not hastened death by assisted suicide.
We’ve seen here that Minnesota’s assisted suicide bill manipulates language in an attempt to make causing a patient’s death an acceptable form of medical care.
Compassion & Choices and other advocates behind this bill are trying to prohibit calling assisted suicide exactly what it is. Assisted Suicide advocates can try to require physicians to falsify death certificates, but this will only undermine the knowledge needed to provide patients with real medical care. Finally, leaving loopholes in this bill’s language, that fail to protect medical professionals and facilities against coercive participation, may ultimately force well-qualified medical professionals from their field, thereby compromising patient care.
Minnesotans deserve laws that uphold the true meaning of medical care, not laws that equate causing death and care. Minnesotans deserve laws that provide the facts necessary for to good public health, not falsified death certificates. Minnesotans deserve laws that protect their doctors and healthcare facilities from lawsuits that would force them out of the medical field.
Minnesotans deserve real care throughout life’s journey not hastened death by assisted suicide.